We Offer Telemedicine Appointments.
Parkinson's Disease
Symptoms, Stages & Causes
What is Parkinson's Disease?
Parkinson’s disease is a neurodegenerative condition in which dopamine-producing nerve cells in the brain become damaged and die, resulting in symptoms such as tremor, stiffened muscles, cognitive impairment, fatigue, difficulty walking, and impaired speech.
Dopamine is a chemical compound produced in the brain that functions as a neurotransmitter. This means that it transmits signals between nerve cells (neurons) and the brain. Not all neurons produce dopamine (only around 400,000 of 85 billion!) and those that do, also called dopaminergic neurons, are found in certain areas of the brain including:
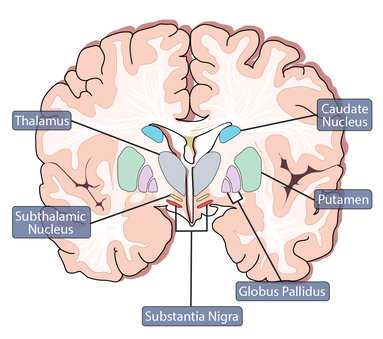
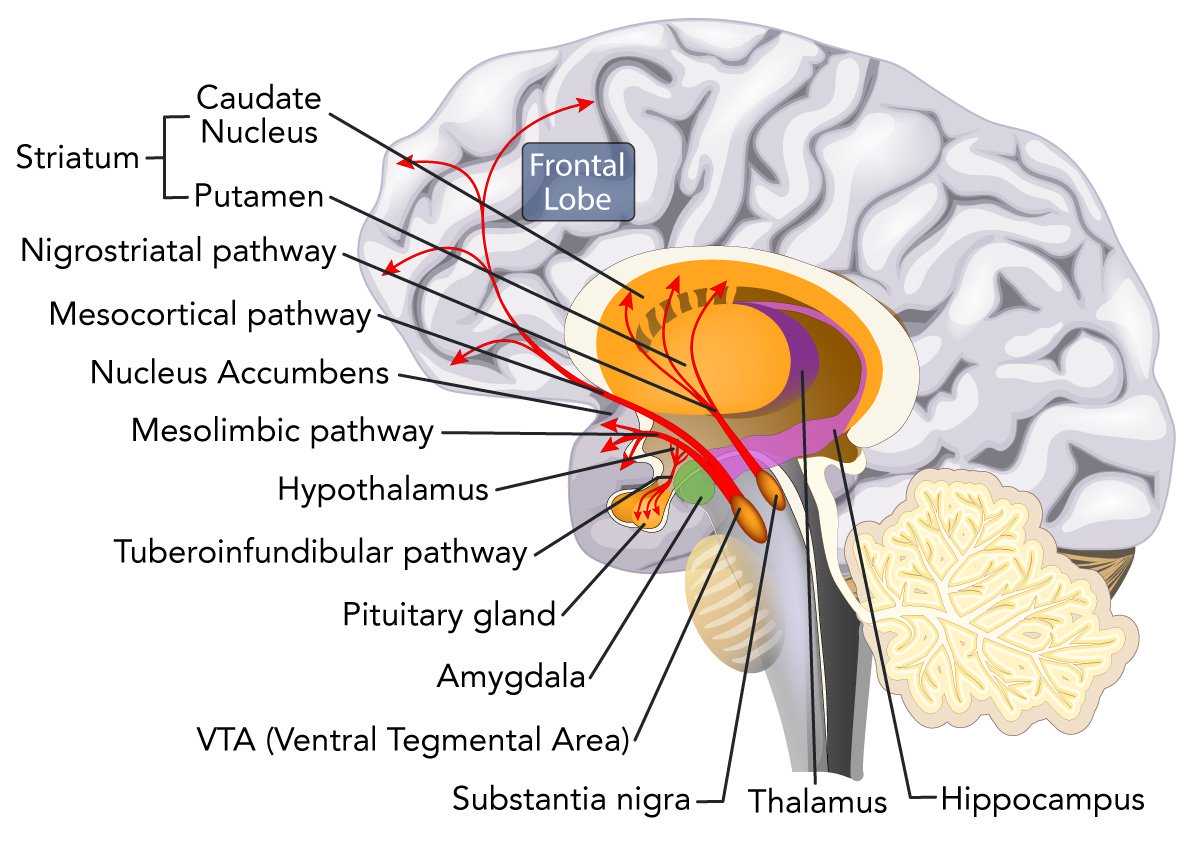
- Substantia nigra: Located in the midbrain, the substantia nigra is a nucleus composed of two distinct parts; the pars compacta and pars reticulata. A majority of the dopaminergic neurons are found in the pars compacta and the pars reticulata facilitates the movement of dopamine using GABA neurons. The nigrostriatal pathway transport dopamine from the Substantia Nigra to the Putamen and Caudate Nucleus, together referred to as the Striatum (see picture Dopamine Pathways).

Normal State

Parkinson's Disease
- Ventral tegmental area: The VTA is also located in the midbrain area, close to the substantia nigra. It possesses a variety of neurons, however, the majority of them are dopaminergic. Although there are other pathways that transport dopamine from the VTA throughout the brain, two major pathways include the mesocortical and mesolimbic. The mesocortical pathway extends into the prefrontal cortex while the mesolimbic pathway projects into the hippocampus, amygdala, and nucleus accumbens.
- Hypothalamus: The hypothalamus is a small region of the brain located between the thalamus and the pituitary gland. Dopamine is produced in the hypothalamus’ arcuate nucleus. and transported into the pituitary gland through the tuberoinfundibular pathway.
Dopamine Pathways
The Role of Dopamine
Dopamine plays important roles in the human body including:
Reward seeking behavior
Rewards can be acts, events, or stimuli that for a variety of reasons (evolutionarily or chemically) increase utility or pleasure and the release of dopamine in the brain. Primary rewards are those that help propagate the species such as food, water, sex, and a safe environment. Non Primary rewards are monetarily, socially, or subjectively derived. They can on deeper analysis be evolutionarily advantageous but they generally require incurring an immediate cost or sacrifice for delayed gratification, making them distinct from primary rewards. Rewards can also be categorized as intrinsic or extrinsic. Intrinsic rewards are those that are for internally derived for oneself and bear similarities to non primary rewards (passions, art, exercise, reading, and exploration). Extrinsic rewards are those reliant on a stimuli or events outside of oneself, generally materialistic or societal, bearing similarities to primary and non primary rewards. All rewards can be conditioned or learned.
Due to the pleasurable effects that primary and secondary rewards have on the brain they can lead to reward-seeking behaviors including consummatory and approach behaviors (the act of getting closer to the reward). The more frequently a reward is attained and dopamine is released, eventually the brain begins to adjust by producing less dopamine (tolerance).
Memory functions
Dopamine affects long-term episodic memory - memories of consecutive events, places, and emotions. It helps the brain consolidate events in the long-term memory where they become strongly ingrained.
Cognition and attention
Dopamine in the prefrontal cortex - the region of the brain responsible for cognitive behavior, social behavior, and the expression of personality - modulates three specific aspects of cognitive control. These are gating (filtering out of unnecessary information), maintaining (manipulating the contents of functioning memory), and relaying (transmitting motor signals).
Pain processing
Dopamine modulates pain perception. Although the exact mechanism is not known, studies show that patients who have a lower than normal level of dopamine - such as those suffering from Parkinson’s disease - often have an abnormally sensitive perception of pain.
Types of Parkinson's Disease
Parkinsons generally occurs between the ages of 50 and 65, however, if PD occurs before the age of 50 this is referred to as Young Onset Parkinson's Disease. Parkinson's Disease is commonly confused with Parkinsonism, which are disorders that mimic PD symptoms.
Young Onset Parkinson’s Disease (YOPD)
YOPD occurs in people under the age of 50. It affects between 10 and 20 percent of people with Parkinson’s disease. People who have several family members with Parkinson’s disease have an increased risk of YOPD. Head trauma may also be a risk factor. People with YOPD are more likely to experience symptoms of dystonia and dyskinesia (due to medication treatment using Levodopa). Dystonia causes involuntary contractions of the muscles that cause the affected body part to twist abnormally. Dyskinesia causes sudden, involuntary muscle spasms which result in jerking body movements or tics. People with YOPD tend to be less likely to experience symptoms such as problems with gait, balance, or dementia.
Types of Parkinsonism
Parkinson's disease should not be confused with Parkinsonism, also called Parkison’s syndrome,
Atypical Parkinsonism Disorder, or Parkinson’s Plus. Parkinsonism refers to a group of neurodegenerative disorders that produce motor problems similar to those caused by Parkinson’s Disease. These disorders include:
- Drug-Induced Parkinsonism (DIP): After Parkinson’s disease, this is the most commonly diagnosed of the Parkinson-like neurodegenerative disorders in elderly people. Often patients with this condition may be misdiagnosed with Parkinson’s disease because the signs and symptoms are so similar. DIP is caused by dopamine agonists (medications which block the function of dopamine). These include some antipsychotic medications, dopamine depletors, SSRIs (serotonin reuptake inhibitors), and neuroleptics (a type of tranquiliser). Treatment for DIP usually involves identifying the offending medication and exchanging it for one which will not have the same effects on dopamine levels.
- Multiple System Atrophy (MSA): A rare neurodegenerative disease that is caused by damage and death of nerve cells in the spinal cord and brain. It affects the autonomic nervous system (which regulates normal homeostatic bodily functions including but not limited to heart rate, perspiration, urination, sexual arousal, and digestion) and motor functions. Symptoms include difficulty walking, problems with balance, and stiffened muscles, urinary incontinence, and erectile dysfunction, among other symptoms. The aim of treatment for MSA is to manage symptomatology.
- Progressive Supranuclear Palsy (PSP): A rare progressive disorder that affects many motor functions including swallowing, gait, vision, and speech as well as cognitive functions, mood, and behavior. It is caused by the death of nerve cells in the brain. There is no specific treatment for PSP, so the goal is to manage symptoms.
- Vascular Parkinsonism: This is caused by blood clots in the brain which are a result of several mini strokes. The condition mainly affects the lower body and causes difficulty walking. Unfortunately, treating vascular parkinsonism with the medications typically used to treat Parkinson’s disease is rarely effective. The goal of treatment is to reduce the risk of further strokes as much as possible. This can include living a healthy lifestyle (exercise/ healthy diet), using blood thinners, and stopping smoking.
- Dementia with Lewy bodies (DLB): This condition is a form of progressive dementia and is the second most commonly diagnosed form of dementia after Alzheimer’s disease. It is caused by abnormal protein deposits in the brain that form into masses - these are called Lewy bodies after the German neurologist who discovered them. The reason Lewy bodies appear in the brain is not known, however, these deposits obstruct neurotransmissions, chemical balances, and eventually lead to nerve death. Symptoms may include problems with movement and cognitive functions. The aim of treatment is to manage symptoms with medication and therapy.
- Corticobasal Syndrome (CBS): This is the least common type of Parkinsonism. Symptoms include imparied cognitive functions (usually arising before motor issues) and impaired motor skills. There is no treatment to slow the advance of this condition and unfortunately, the symptoms do not typically respond well to therapy.
- Essential tremor (ET): The cause of this type of Parkinsonism is not known, although it is hereditary in around 50 percent of cases. ET is more apparent when a person is moving rather than when at rest and can affect gait and fine manual movements or tasks (such as using a pencil or utensil). Treatment usually involves medications such as tranquilizers, beta blockers (propranolol), anti-seizure drugs, and botulinum toxin injections (for muscle spasms). If the tremors are particularly debilitating, surgery may be an option. Surgical options include Gamma Knife thalamotomy, focused ultrasound thalamotomy, and deep brain stimulation.
- Normal pressure hydrocephalus (NSA): NSA is a disorder in which an excess of cerebrospinal fluid (CSF) causes enlargement of the ventricles in the brain. The symptomatology of NSA is similar to Vascular Parkinsonism and includes mild cognitive impairment, such as forgetfulness, difficulty walking, problems with balance, and loss of bladder control (as the condition progresses). Treatment involves the placement of a shunt in the brain to drain the excess CSF.
If you or someone you love has been diagnosed with Parkinson's Disease, there is help.
It is our aim at Miami Neuroscience Center at Larkin to treat this condition cost-effectively while providing high-quality care and optimal outcomes. Explore all of our treatment options and meet the top Parkinson's specialists in Miami, call us today to learn more about managing your symptoms.
Parkinson’s Symptoms
The signs and symptoms of Parkinson’s disease can differ from person to person. During the initial stages of the disease, symptoms may be so slight that they are not noticed. Around 80 percent of individuals who are diagnosed with Parkinson’s disease have idiopathic Parkinson’s disease, also called primary parkinsonism. Parkinson’s disease symptoms may include:

Involuntary tremors affect around 80% of sufferers. In most cases, Parkinson’s tremor can be treated successfully with medication. Tremors can occur in the hands, fingers, arms, legs, feet, jaw, vocal cords, lip, or torso. There are two types of Parkinson’s tremors:
Resting tremor: This is the most common form of tremor in Parkinson’s disease. Resting tremors occur when the patient is at rest, such as sitting in a chair with their hands on their lap, or when they are in bed. Movement will cause the tremor to go away. Resting tremors cause uncontrollable shaking or rubbing of a limb, such as the hands, feet, or fingers. Rubbing the forefinger and thumb together- known as pill-rolling, is also a sign of resting tremor. Resting tremors are often the first symptom of Parkinson’s disease that causes people to seek medical advice.
Action tremors: Although action tremors are less common than resting tremors, they may affect more than 25 percent of Parkinson’s patients. This type of uncontrollable tremor occurs along with any form of movement and will depend on the part of the body that is being moved.

Bradykinesia is a term used to describe slow movement in Parkinson’s disease. It can slow down general movement, cause difficulty with performing specific movement (such as standing from sitting) or impair autonomic movements (such as blinking).

The manner of walking in most Parkinson’s patients is a small, shuffling steps. The back, shoulders, and head are often bent forward. Many sufferers have difficulty getting started, and once started, difficulty stopping.

Stiffness can affect any of the limbs or the torso and can cause discomfort or pain

In some people speech becomes slower and slurred, while in others it speeds up. It may also be impeded by stammering or stuttering.

It is common for Parkinson’s sufferers to experience issues throughout their gastrointestinal tract. These may include difficulty swallowing, gastroparesis (the stomach has difficulty emptying), bloating, nausea, and constipation.

Sufferers may become more introverted, they may develop compulsive behaviors, or they may begin to act impulsively.

Studies demonstrating the prevalence of psychosis in patients with Parkinson’s disease vary due to factors including treatment approach, PD stage, and assessment criteria. However, some studies estimate that up to 40 percent of people with Parkinson’s disease will develop psychosis. Symptoms typically include hallucinations and/or delusions.

Dystonia involves involuntary muscle spasms which cause the affected part of the body to twist into an abnormal position. It can affect the limbs, neck, arms, torso, and eyes.

Loss of taste and smell are often early symptoms of Parkinson’s disease.
Parkinson’s Disease Causes
The exact cause of Parkinson’s disease is not known. However, contributing factors may include certain gene mutations which may in rare cases occur in people who have several family members who suffer from Parkinson’s disease. Environmental factors such as exposure to toxic chemicals like pesticides and head injury may also increase a person's chance of developing Parkinson’s disease.
Parkinson’s Disease Risk Factors
- Age: In most cases, people do not develop noticeable signs of Parkinson’s disease until they are 60 or older. Only in about 10 percent of cases or less do people develop early onset Parkinson’s disease (before 50 years of age).
- Gender: Men are twice as likely to develop Parkinson’s than women. In addition, women tend to be on average two years older than men they develop PD.
- Family history: Around 15 percent of people with Parkinson’s have a family member with this condition.
- Ethnicity: Hispanics and Caucasions have the highest incidence of Parkinson’s disease while African Americans and Asians have the lowest incidence.
FAQ - Parkinson’s Disease Frequently Asked Questions
Alzheimer’s disease is the most common type of dementia; around 70% of people with Dementia have Alzheimer’s Disease. Whereas dementia may occur in some cases of Parkinson’s but this is not an inevitable outcome. Dementia occurs in around 50-80% of cases of Parksinon’s disease and it generally takes a decade or more to develop.
| Parkinson’s Disease | Alzheimer’s Disease | |
|---|---|---|
| Cause | Decreased Dopamine Production | Build-up of beta-amyloid plaques & neurofibrillary tangles |
| Symptoms | Distinct Motor Impairments (tremors, slowness, and rigidity) & Some Cognitive Impairments similar to Alzheimers | Cognitive Impairments (memory loss and personality changes) |
| Age Onset | ~50-65 | ~62+ |
| Prevalence by 2020 | Less Common (~1 million) | More Common (~5.8 million) |
| Gender | Male > Female | Female > Male |
| Ethnicities Affected | Hispanics and Caucasians | Hispanics and African Americans |
By 2020, it is estimated that Parkinson’s disease will affect about a million Americans. Due to the increasingly aging population in the US, the number of people with PD is expected to grow.
These conditions are not the same. PSP is a form of Parkinsonism. It is a rare condition that causes motor and cognitive problems. See a description of PSP by clicking here.
People who suffer from this condition tend to have a slightly shorter life span than people of the same age who are not sufferers. Parkinson’s disease is a progressive disorder, but it is not considered to be a fatal condition.
Around 15% of sufferers have family members with this condition which is called Hereditary Parkinson’s.
Signs and symptoms of Parkinson's Disease are different for each person, however, some symptoms may include tremors, slowness and difficulty moving, balance problems, speech impairment, cognitive decline, and hallucinations.
One: Symptoms are mild. Motor symptoms only occur on one side of the body.
Two: Symptoms worsen. Motor symptoms may now affect both sides of the body.
Three: This is the mid-stage. Loss of balance is more common and falls are frequent.
Four: Symptoms are severe. A walker may be needed.
Five: Symptoms become debilitating. Around-the-clock care is needed.
Parkinsonism is not the same as Parkinson’s disease. Parkinsonism is a group of Parkinson-like disorders that may share some of the same symptoms.
References
Neuroscientifically Challenged "Know your brain: Substantia nigra" November 2014. https://www.neuroscientificallychallenged.com/blog/know-your-brain-substantia-nigra
ScienceDirect "Mesocortical Pathway" https://www.sciencedirect.com/topics/neuroscience/mesocortical-pathway
Wolfram Schultz "Neuronal Reward and Decision Signals: From Theories to Data" National Center for Biotechnology Information (NCBI), June 2015. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4491543/
Arias-Carrión O; Pŏppel E. "Dopamine, learning, and reward-seeking behavior" National Center for Biotechnology Information (NCBI), February 2007. https://www.researchgate.net/publication/5531082_Dopamine_learning_and_reward-seeking_behavior
Grogan, John; Bogacz, Rafal; Tsivos, Demitra; Whone, Alan; Coulthard, Elizabeth "Dopamine and Consolidation of Episodic Memory: Timing Is Everything" Journal of Cognitive Neuroscience, June 2015. https://research-information.bristol.ac.uk/en/publications/dopamine-and-consolidation-of-episodic-memory(425b3cab-ecec-4fce-ba74-a3471ffd0779).html
Torben Ott; Andreas Nieder "Dopamine and Cognitive Control in Prefrontal Cortex" Elsevier, January 2019. https://www.cell.com/trends/cognitive-sciences/fulltext/S1364-6613(19)30013-0
National Institute of Neurological Disorders and Stroke (NINDS) "Tremor Fact Sheet" May 2017. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Tremor-Fact-Sheet#5
Raquel N. Taddei; Seyda Cankaya; Sandeep Dhaliwal; K. Ray Chaudhuri "Management of Psychosis in Parkinson's Disease: Emphasizing Clinical Subtypes and Pathophysiological Mechanisms of the Condition" National Center for Biotechnology Information (NCBI), Septemebr 2017. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5613459/
The Parkinson's Foundation "Young Onset Parkinson's" https://www.parkinson.org/Understanding-Parkinsons/What-is-Parkinsons/Young-Onset-Parkinsons
The Michael J. Fox Foundation For Parkinson's Research "Young-Onset Parkinson's Disease" https://www.michaeljfox.org/news/young-onset-parkinsons-disease
Hae-Won Shina; Sun Ju Chung "Drug-Induced Parkinsonism" National Center for Biotechnology Information (NCBI), March 2012. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3325428/
The Parkinson's Foundation "Parkinson’s Disease vs. Parkinsonism" 2018. https://parkinson.org/sites/default/files/attachments/Parkinsons-Disease-vs-Parkinsonisms.pdf
National Institute of Health (NIH) "Parkinson's Disease" May 2017. https://www.nia.nih.gov/health/parkinsons-disease
Lyons KE; Hubble JP; Tröster AI; Pahwa R, Koller WC "Gender differences in Parkinson’s disease" National Center for Biotechnology Information (NCBI), March 1998. https://www.ncbi.nlm.nih.gov/pubmed/9579298
National Institute of Health (NIH) "Parkinson's Disease: Hope Through Research" December 2014. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Hope-Through-Research/Parkinsons-Disease-Hope-Through-Research
To learn more about Parkinson's Disease and to see how we can help you please call us at 786.871.6856 or schedule a consultation today!